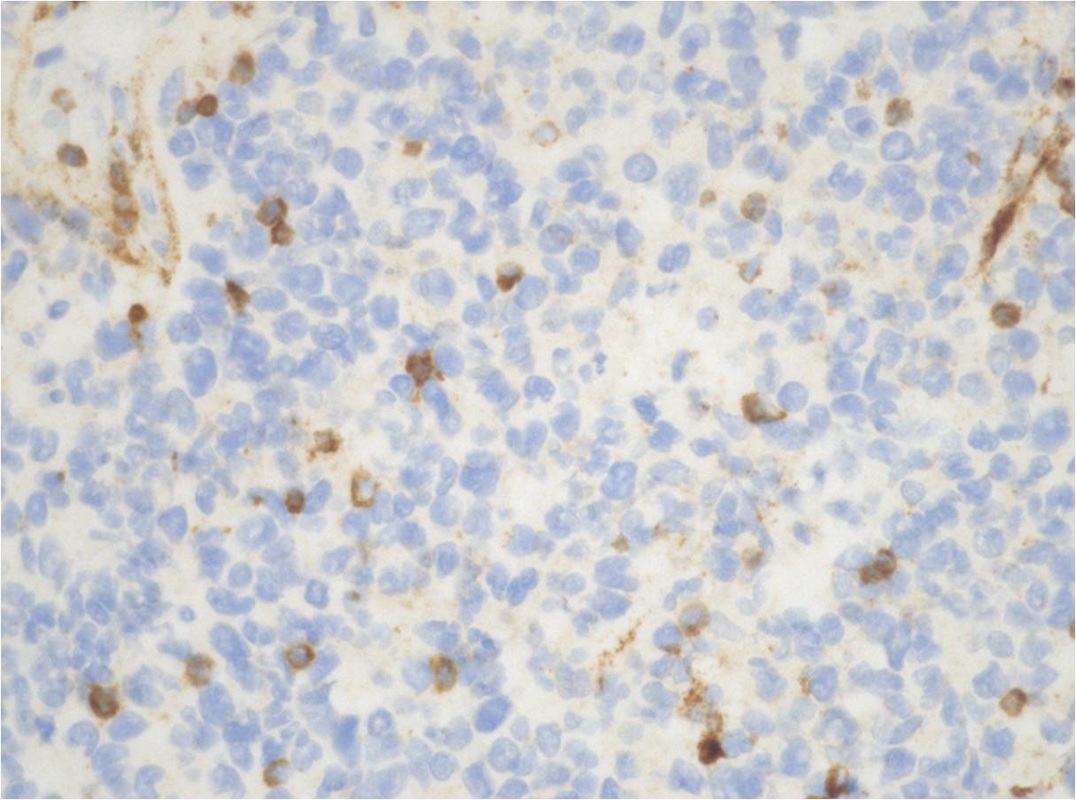
Immunostains:






Flow cytometry: 30% B cells with no surface light chains.
Diagnosis: Primary mediastinal large B-cell lymphoma
Diagnosis: Primary mediastinal large B-cell lymphoma
Primary mediastinal (thymic) large B-cell lymphoma
Epidemiology: 2-4% of non-Hodgkin-lymphomas (NHL), predominantly in young adults (median age, ~35 years) with a female predominance (M:F ratio, about 1:2).
Sites: anterosuperor mediastinal mass. No BM involvement. Symptom related to mass effect, and possible B symptom.
Morphology: wide morphological/cytological spectrum, commonly compartmentalizing alveolar fibrosis. Tumour cells: medium-sized to large cells with abundant pale cytoplasm and more or less regular round or ovoid nuclei. occasional pleomorphic multilobated nuclei (mimick Hodgkin cells).
Immunophenotype: Positive for B-cell antigens such as CD19, CD20, CD22 and CD79a, but lacks immunoglobulin (Ig). CD30 is present in more than 80% of the cases, usually weak and heterogeneous. CD15 is occasionally present. Frequently positive for IRF4/MUM1 (75%) and CD23 (70%), have variable expression of BCL2 (55-80%) and BCL6 (45-100%) and CD10 is less common (8-32%). Positive for MAL antigen, CD54 and CD95, coexpress TRAF1 and nuclear REL.
Antigen receptor genes: Immunoglobulin genes are clonally rearranged with a high load of somatic hypermutations without ongoing mutational activity.
Cytogenetic and oncogene abnormalities: CGH demonstrated gains in chromosome 9p24 (up to 75%) and 2p15 (~50%), but also in chromosomes Xp11.4-21 (33%) and Xq24-26 (33%). Candidate genes: REL and BCL11A (at 2p),and JAK2, PDL1 and PDL2 (at 9p); transcriptional signature shares features with CHL.
Rearrangements of BCL2, BCL6 and MYC genes are absent or rare. Inactivation of p16INK4a and TP53 genes have been reported.
Epidemiology: 2-4% of non-Hodgkin-lymphomas (NHL), predominantly in young adults (median age, ~35 years) with a female predominance (M:F ratio, about 1:2).
Sites: anterosuperor mediastinal mass. No BM involvement. Symptom related to mass effect, and possible B symptom.
Morphology: wide morphological/cytological spectrum, commonly compartmentalizing alveolar fibrosis. Tumour cells: medium-sized to large cells with abundant pale cytoplasm and more or less regular round or ovoid nuclei. occasional pleomorphic multilobated nuclei (mimick Hodgkin cells).
Immunophenotype: Positive for B-cell antigens such as CD19, CD20, CD22 and CD79a, but lacks immunoglobulin (Ig). CD30 is present in more than 80% of the cases, usually weak and heterogeneous. CD15 is occasionally present. Frequently positive for IRF4/MUM1 (75%) and CD23 (70%), have variable expression of BCL2 (55-80%) and BCL6 (45-100%) and CD10 is less common (8-32%). Positive for MAL antigen, CD54 and CD95, coexpress TRAF1 and nuclear REL.
Antigen receptor genes: Immunoglobulin genes are clonally rearranged with a high load of somatic hypermutations without ongoing mutational activity.
Cytogenetic and oncogene abnormalities: CGH demonstrated gains in chromosome 9p24 (up to 75%) and 2p15 (~50%), but also in chromosomes Xp11.4-21 (33%) and Xq24-26 (33%). Candidate genes: REL and BCL11A (at 2p),and JAK2, PDL1 and PDL2 (at 9p); transcriptional signature shares features with CHL.
Rearrangements of BCL2, BCL6 and MYC genes are absent or rare. Inactivation of p16INK4a and TP53 genes have been reported.
