Cytochemical stains:

Flow cytometry study:
An aberrant population is present and the cells are positive for CD7, CD71 and Glycophorin A and negative for CD45 and other myeloid and lymphoid markers.
An aberrant population is present and the cells are positive for CD7, CD71 and Glycophorin A and negative for CD45 and other myeloid and lymphoid markers.
Diagnosis: Acute erythroid leukemia (AML M6)
Changes have been made in 2016 revised WHO classification:
The subcategory of acute erythroid leukemia, erythroid/myeloid type (previously defined as a case with ≥50% BM erythroid precursors and ≥20% myeloblasts among nonerythroid cells) has been removed from the AML category. In the new classification, myeloblasts are always counted as a percentage of total marrow cells and the majority of such cases have <20% total blast cells and are now classified as MDS (usually MDS with excess blasts). This change was based on the close biologic relationship of erythroid/myeloid type acute erythroid leukemia to MDS in terms of its clinical presentation, morphologic features, and genetic abnormalities, as well as the low reproducibility of nonerythroid blast counts and an attempt to achieve uniformity in expressing blast percentages across all myeloid neoplasms. Cases with ≥50% or more erythroid cells and ≥20% total myeloblasts usually meet criteria for AML with myelodysplasia-related changes and should be diagnosed as such; cases with ≥ 20%total myeloblasts not meeting criteria for AML with myelodysplasia-related changes or AML with recurrent genetic abnormalities should be categorized as 1 of the other subtypes of AML, NOS. Pure erythroid leukemia remains as an AML, NOS subtype and is now the only type of acute erythroid leukemia.
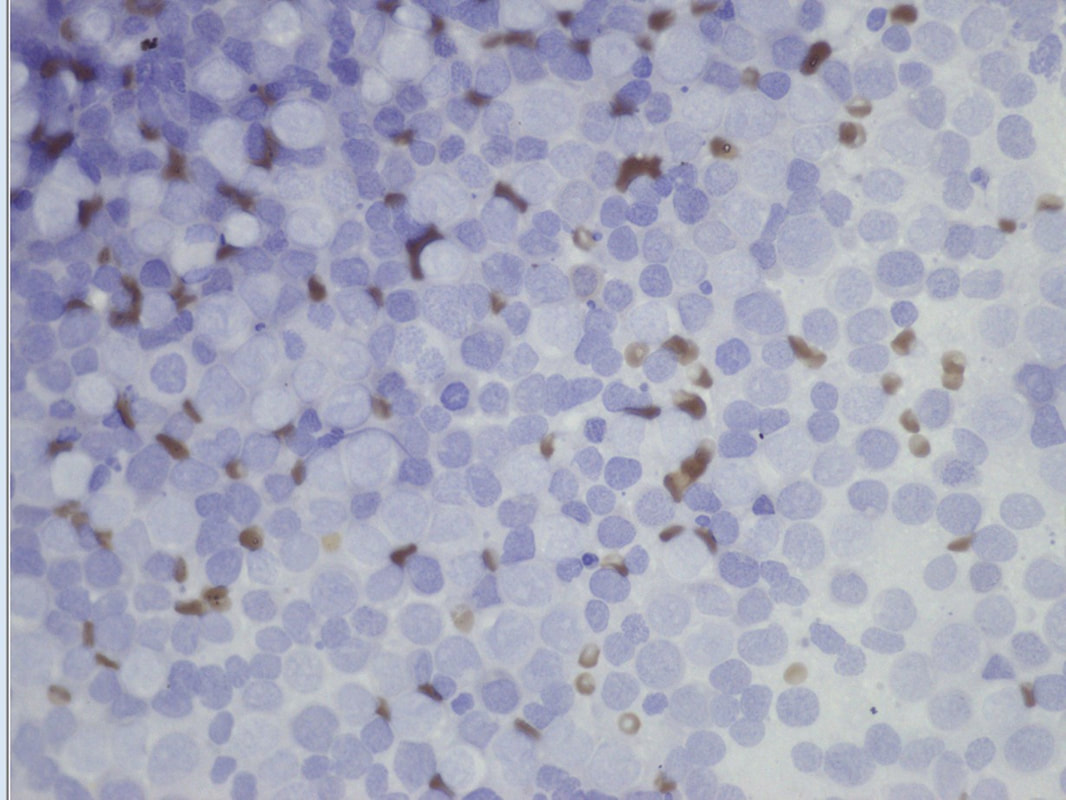
Pure erythroid leukaemia represents a neoplastic proliferation of immature cells (undifferentiated or eroerythroblastic in appearance) committed exclusively to the erythroid lineage (>80% of BM cells, >% proerythroblasts) with no evidence of a significant myeloblastic component. Pure erythroid leukaemia is extremely rare and can occur at any age, including childhood. The undifferentiated form of pure erythroid leukaemia is usually characterized by the presence of medium to large size rythroblasts usually with round nuclei, fine chromatin and one or more nucleoli(proerythroblast); the cytoplasm is deeply basophilic, often agranular and frequently contains poorly demarcated vacuoles which are often PAS-positive. Occasionally the blasts are smaller and resemble the lymphoblasts of ALL. The cells are negative for MPO and SBB; they show reactivity with α-naphthyl acetate esterase, acid phosphatase and PAS, the latter usually in a block-like staining pattern. In the BM biopsies of pure acute erythroid leukaemia the cells appear undifferentiated. The more differentiated forms can be detected by the expression of glycophorin and haemoglobin A and absence of MPO and other myeloid markers; the blasts are often negative for HLA-DR and CD34, but may be positive for CD117. The more immature forms are usually negative for glycophorin or this is only weakly expressed in a minority of blasts. Other markers such as carbonic anhydrase 1, Gero antibody against the Gerbich blood group or CD36 are usually positive as they detect erythroid progenitors at earlier stages of differentiation. However, CD36 is not specific for erythroblasts and may be ex-pressed by monocytes and megakaryocytes. Antigens associated with megakaryocytes (CD41 and CD61) are typically negative, but may be partially expressed in some cases. Immunohistochemistry to haemoglobin A or glycophorin may be helpful in establishing cell origin in biopsy specimens.
Changes have been made in 2016 revised WHO classification:
The subcategory of acute erythroid leukemia, erythroid/myeloid type (previously defined as a case with ≥50% BM erythroid precursors and ≥20% myeloblasts among nonerythroid cells) has been removed from the AML category. In the new classification, myeloblasts are always counted as a percentage of total marrow cells and the majority of such cases have <20% total blast cells and are now classified as MDS (usually MDS with excess blasts). This change was based on the close biologic relationship of erythroid/myeloid type acute erythroid leukemia to MDS in terms of its clinical presentation, morphologic features, and genetic abnormalities, as well as the low reproducibility of nonerythroid blast counts and an attempt to achieve uniformity in expressing blast percentages across all myeloid neoplasms. Cases with ≥50% or more erythroid cells and ≥20% total myeloblasts usually meet criteria for AML with myelodysplasia-related changes and should be diagnosed as such; cases with ≥ 20%total myeloblasts not meeting criteria for AML with myelodysplasia-related changes or AML with recurrent genetic abnormalities should be categorized as 1 of the other subtypes of AML, NOS. Pure erythroid leukemia remains as an AML, NOS subtype and is now the only type of acute erythroid leukemia.
Pure erythroid leukaemia represents a neoplastic proliferation of immature cells (undifferentiated or eroerythroblastic in appearance) committed exclusively to the erythroid lineage (>80% of BM cells, >% proerythroblasts) with no evidence of a significant myeloblastic component. Pure erythroid leukaemia is extremely rare and can occur at any age, including childhood. The undifferentiated form of pure erythroid leukaemia is usually characterized by the presence of medium to large size rythroblasts usually with round nuclei, fine chromatin and one or more nucleoli(proerythroblast); the cytoplasm is deeply basophilic, often agranular and frequently contains poorly demarcated vacuoles which are often PAS-positive. Occasionally the blasts are smaller and resemble the lymphoblasts of ALL. The cells are negative for MPO and SBB; they show reactivity with α-naphthyl acetate esterase, acid phosphatase and PAS, the latter usually in a block-like staining pattern. In the BM biopsies of pure acute erythroid leukaemia the cells appear undifferentiated. The more differentiated forms can be detected by the expression of glycophorin and haemoglobin A and absence of MPO and other myeloid markers; the blasts are often negative for HLA-DR and CD34, but may be positive for CD117. The more immature forms are usually negative for glycophorin or this is only weakly expressed in a minority of blasts. Other markers such as carbonic anhydrase 1, Gero antibody against the Gerbich blood group or CD36 are usually positive as they detect erythroid progenitors at earlier stages of differentiation. However, CD36 is not specific for erythroblasts and may be ex-pressed by monocytes and megakaryocytes. Antigens associated with megakaryocytes (CD41 and CD61) are typically negative, but may be partially expressed in some cases. Immunohistochemistry to haemoglobin A or glycophorin may be helpful in establishing cell origin in biopsy specimens.

Blood. 2016; 127(20):2391-2405
