More history: pt swam in freshwater lake.
Diagnosis: Primary amebic meningoencephalitis
Amebic meningoencephalitis is caused by free-living amebas, predominately Naegleria fowleri and Acanthamoeba spp.
Naegleria fowleri meningoencephalitis (primary amebic meningoencephalitis) affects children and young adults, acquired by swimming in fresh water, and is almost always fatal. Infections are spread through the nose. Naegleria species are found in large numbers in shallow fresh water, particularly during warm weather. Among 140 cases reported, only 4 people survived with treatment with high-dose amphotericin B along with rifampin. Symptoms can be mild at first, but they worsen quickly. Usually start about 5 days after infection (but can range from 1–7 days); Can include headache, fever, nausea, or vomiting; Later symptoms can include stiff neck, confusion, lack of attention to people and surroundings, loss of balance, seizures, and hallucinations; After symptoms start, the disease causes death within about 5 days.
Diagnosis: Primary amebic meningoencephalitis
Amebic meningoencephalitis is caused by free-living amebas, predominately Naegleria fowleri and Acanthamoeba spp.
Naegleria fowleri meningoencephalitis (primary amebic meningoencephalitis) affects children and young adults, acquired by swimming in fresh water, and is almost always fatal. Infections are spread through the nose. Naegleria species are found in large numbers in shallow fresh water, particularly during warm weather. Among 140 cases reported, only 4 people survived with treatment with high-dose amphotericin B along with rifampin. Symptoms can be mild at first, but they worsen quickly. Usually start about 5 days after infection (but can range from 1–7 days); Can include headache, fever, nausea, or vomiting; Later symptoms can include stiff neck, confusion, lack of attention to people and surroundings, loss of balance, seizures, and hallucinations; After symptoms start, the disease causes death within about 5 days.

Organism Description:
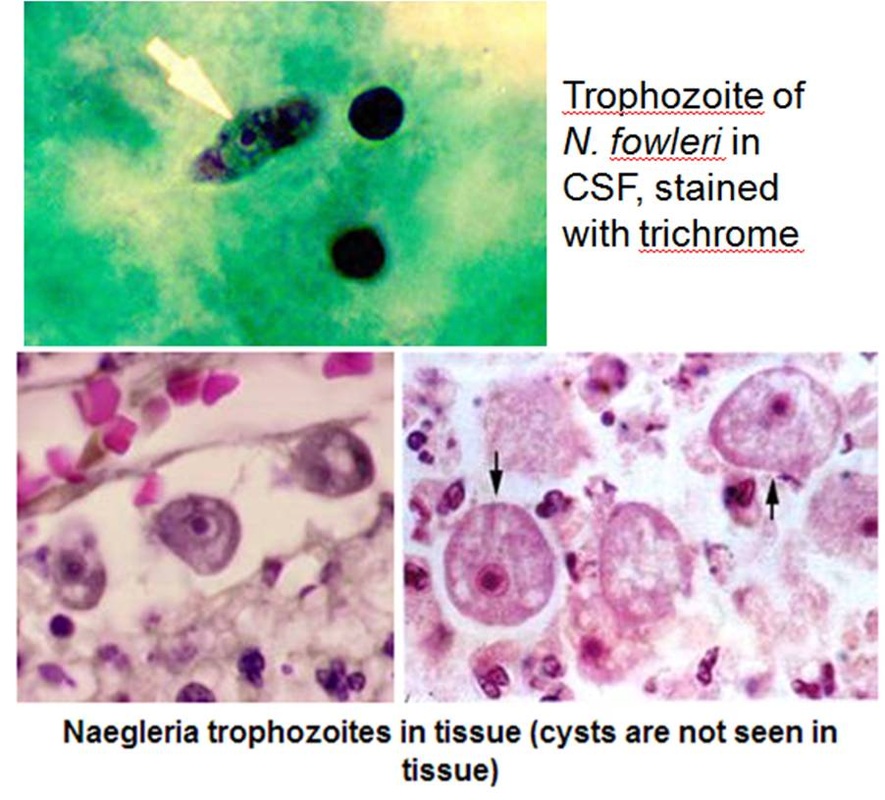
Trophozoite: the ameboid form (the only form recognized in humans) is elongate with a broad anterior end and tapered posterior end. The size ranges from 7 to 35 μm. The diameter of the rounded forms is usually 15 μm. There is a large, central karyosome and no peripheral nuclear chromatin. The cytoplasm is somewhat granular and contains vacuoles. The ameboid‑form organisms change to the transient, pear‑shaped flagellate form when they are transferred from culture or teased from tissue into water and maintained at a temperature of 27 to 37°C. The change may occur very quickly (within a few hours) or may take as long as 20 h. The flagellate form has two flagella at the broad end. Motility is typical, with either spinning or jerky movements. These flagellate forms do not divide, but when the flagella are lost, the ameboid forms resume reproduction.
Cyst: The cyst typically has a double wall and can be seen in culture, but not in tissue or the CSF.
Trophozoite: the ameboid form (the only form recognized in humans) is elongate with a broad anterior end and tapered posterior end. The size ranges from 7 to 35 μm. The diameter of the rounded forms is usually 15 μm. There is a large, central karyosome and no peripheral nuclear chromatin. The cytoplasm is somewhat granular and contains vacuoles. The ameboid‑form organisms change to the transient, pear‑shaped flagellate form when they are transferred from culture or teased from tissue into water and maintained at a temperature of 27 to 37°C. The change may occur very quickly (within a few hours) or may take as long as 20 h. The flagellate form has two flagella at the broad end. Motility is typical, with either spinning or jerky movements. These flagellate forms do not divide, but when the flagella are lost, the ameboid forms resume reproduction.
Cyst: The cyst typically has a double wall and can be seen in culture, but not in tissue or the CSF.

•Left: EM image of Naegleria fowleri in its cyst stage. Center: EM image of Naegleria fowleri in its ameboid trophozoite stage. Right: EM image of Naegleria fowleri in its flagellated stage. Credit:DPDx and GS Visvesvara.
Diagnosis: A careful examination of the cerebrospinal fluid often provides a presumptive diagnosis of Naegleria infection. The fluid is usually bloody and demonstrates an intense neutrophilic response with trophozoites with foamy cytoplasm. The protein level is elevated and the glucose level decreased. Specimen should not be refrigerated before examination. Early examination of a wet mount preparation can show the typical trophozoites. Fluorescent staining or culture can confirms the identification.

|
|
Acanthamoeba meningoencephalitis usually involves older, immunocompromised persons, it is subacute or chronic, fatal or occasional self-recovery. They are found in soil and in fresh and brackish water. It reaches the brain by hematogenous dissemination from an unknown primary site, possibly the respiratory tract, skin, or eye. Histologically, Acanthamoeba infections produce a diffuse, necrotizing, granulomatous encephalitis. Both cysts and trophozoites can be found in the lesions. The spinal fluid usually demonstrates a mononuclear response. Definitive diagnosis is usually made histologically after death. Acanthamoeba species are sensitive to a variety of agents, but studies of clinical efficacy have not been performed.

