IHC Stains:
LN:







Appendix:






Colon and Rectum:


|
Diagnosis:
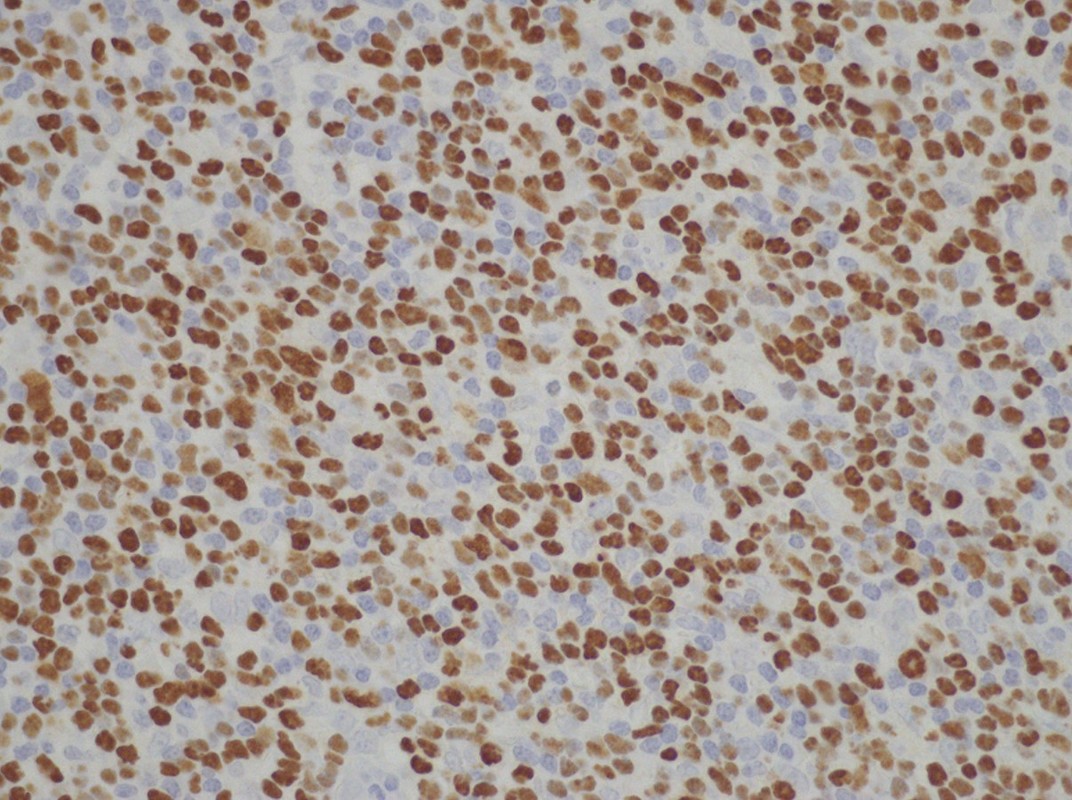
Chronic active EBV infection of T cells. Chronic active EBV infection (CAEBV) of T/NK cells shows a broad range of clinical manifestations. CAEBV was initially defined as a severe illness of greater than 6 months’ duration that (1) begins as a primary EBV infection or is associated with markedly abnormal EBV antibody titers; (2) shows histologic evidence of major organ involvement, such as interstitial pneumonia, hypoplasia of the bone marrow, uveitis, lymphadenitis, persistent hepatitis, or splenomegaly; and (3) exhibits increased EBV RNA or proteins in affected tissues. The initial description of CAEBV did not specify the lineage of the EBV-infected cell, but since then the syndrome has almost always been associated with a proliferation of EBV-infected T cells or NK cells. Most cases consist of a systemic EBV+ polyclonal or oligoclonal T- or NK-cell LPD characterized by a high viral load in peripheral blood and tissues and intermittent or chronic IM–like features such as fever, lymphadenopathy, and hepatosplenomegaly at least 3 months after primary virus infection in patients with no known immunodeficiency. CAEBV infection of B-cell derivation occurs rarely. Chronic persistent IM, which is somewhat more common, represents an illness in which EBV+ B cells persist in significant numbers beyond the acute illness, accompanied by continued clinical symptoms associated with infectious mononucleosis. Because the term CAEBV does not specify the lineage of the EBV-infected cell, a recent international report recommended that the term be modified to include the cellular lineage affected: T cell, NK cell, or B cell. A monoclonal T- or NK-cell lymphoproliferation developing in the setting of CAEBV-T/NK should be diagnosed as malignant lymphoma and classified according to the current WHO classification. Because the infiltrating cells in CAEBV-T/NK are not atypical, it is easy to overlook the diagnosis. In situ hybridization for EBER is a valuable tool for recognizing the disease in the appropriate clinical setting. Systemic EBV+ T-cell LPD or other clearly clonal proliferations must be distinguished from CAEBV-T/NK. In cases with a monoclonal population, the infiltrating cells tend to have increased cytologic atypia and include a higher proportion of EBV+ cells. Because distinction by morphology is difficult, demonstration of the clonality of EBV and EBV-infected T cells is necessary. |

Jaffe ES, et al. Hematopathology. 2011
|

Jaffe ES, et al. Hematopathology. 2011
